The following are common diagnoses of common congenital heart defects we see in adults and recommendations for care for each disease. See a list of the wide variety of other congenital heart conditions we treat at the Michigan Congenital Heart Center at C.S. Mott Children's Hospital.
Tetralogy of Fallot
Tetralogy of Fallot is a relatively common congenital heart disease. Many people with this disease were diagnosed in infancy as “blue babies.” Most patients with Tetralogy of Fallot have undergone surgery in infancy or childhood, and all patients with this heart defect should be evaluated at a dedicated center for the care of adults with congenital heart disease such as the University of Michigan Adult Congenital Heart Program. Patients diagnosed with Tetralogy of Fallot require regular follow-up with a cardiologist, and many patients require repeat surgeries later in life.
Symptoms for Tetralogy of Fallot can include:
- Shortness of breath with activity
- Irregular heart beats
- Loss of consciousness (syncope)
- Abdominal or leg swelling
To learn more about this disease, visit the Tetralogy of Fallot page on the C.S. Mott Children's Hospital website.
Transposition of the Great Arteries
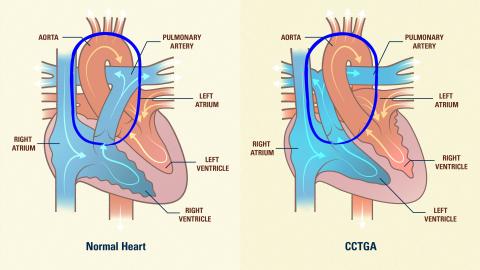
In Transposition of the Great Arteries (TGA), the main pumping chamber of the heart, the left ventricle, gives rise to the pulmonary artery, which supplies the lungs. The right ventricle supplies blood to the body. Babies with Transposition of the Great Arteries can be very cyanotic (blue). Almost all patients with TGA will have undergone some sort of surgery in infancy. Patients in their mid-20’s and younger will generally have undergone arterial switch repair surgery (the University of Michigan was the first hospital in the state of Michigan to perform this surgery), and older patients (mid-20’s and older) will have undergone atrial switch surgeries, known as the Mustard or Senning procedures. Common problems with patients following the Mustard and Senning procedures include heart failure and problems with abnormal heart rhythms.
All patients with TGA require evaluation in a dedicated adult congenital heart program such as the U-M Adult Congenital Heat Program, and patients with TGA requiring pacemakers or other procedures should have them performed at an experienced adult congenital heart center.
To learn more about this disease, visit the Transposition of the Great Arteries page on the C.S. Mott Children's Hospital website.
Atrial Septal Defect
Adults with atrial septal defect may not be diagnosed until their 30’s, 40’s, or 50’s. A heart murmur or the development of abnormal heart rhythms can be the first sign that an atrial septal defect is present, and other symptoms of atrial septal defect can include worsening shortness of breath with activity. Not all atrial septal defects require intervention. Very small defects which do not make the heart enlarge can often just be watched without intervention. Many atrial septal defects can be closed safely without surgery. The University of Michigan Congential Heart Program has a long experience with percutaneous closure of atrial septal defect and was involved with many of the initial studies of safety of closure defects. Larger atrial septal defects, or those in unusual anatomic locations (known as sinus venosus septal defects or primum atrial septal defects) require surgical closure.
To learn more about this disease, visit the Atrial Septal Defect page on the C.S. Mott Children's Hospital website.
Ventricular Septal Defect
Most adults with large ventricular septal defects will have undergone surgical repair in their youth. Patients with repaired or spontaneously closed ventricular septal defects require occasional follow-up in an experienced adult congenital center to evaluate for specific late complications which can occur. Many small ventricular septal defects do not require any time of intervention, although patients with such defects still require life-long follow-up. Patients with large ventricular septal defects who have not undergone surgical repair will develop a significant complication known as Eisenmenger Syndrome. Patients with Eisenmenger syndrome are at extremely high risk with anesthesia for surgery and at the time of pregnancy and should be evaluated at an center experienced in congenital heart disease.
To learn more about this disease, visit the Ventricular Septal Defect page on the C.S. Mott Children's Hospital website.
Ebstein Anomaly
Ebstein Anomaly is a rare form of congenital heart disease affecting the tricuspid valve. Many patients with Ebstein Anomaly also have a hole between their top heart chambers (atrial septal defect). It is common for patients with Ebstein Anomaly to develop abnormal heart rhythms, but many patients with Ebstein Anomaly do not require heart surgery and can do quite well with close observation.
Pulmonary Stenosis
Some patients with pulmonary stenosis require surgery or a catheterization procedure in childhood or infancy, while others may need procedures later in life. Many patients who underwent surgery in childhood for pulmonary stenosis will require repeat procedures later in life for either worsening narrowing of the valve (stenosis), or development of leakage (insufficiency) of the valve. Pulmonary stenosis can often be treated at the time of cardiac catheterization without the need for open heart surgery.
To learn more about this disease, visit the Pulmonary Stenosis page on the C.S. Mott Children's Hospital website.
Single Ventricle Defects and the Fontan Procedure
The Fontan procedure was developed for patients born with only one pumping chamber (ventricle) of their heart. Many patients require surgery prior to their Fontan procedure, which often occurs in early childhood. All patients after a Fontan require evaluation in a dedicated adult congenital heart program such as the University of Michigan Adult Congenital Heart Program. Patients should have close follow-up for development of abnormal heart rhythms, or worsening heart function. Women with the Fontan procedure should undergo extensive evaluation and consultation with an adult congenital heart disease specialist prior to consideration of pregnancy. Symptoms of swelling and chronic diarrhea can be signs of a serious medical problem in Fontan patients and should be evaluated. Patients with the Fontan procedure generally require some type of blood thinner because of the increased risk for blood clots.
Patient Resources
- Adults with Congenital Heart Defects Information Guide
- Heart Rhythm Disorders Information Guide
- Heart Catheterization Information Guide
Make an Appointment
Visit our Make an Appointment page for more information.
For Pediatric Patients
Visit the University of Michigan Pediatric Heart Program at C.S. Mott Children's Hospital online.